Reviewed by Janet D. Pearl, MD, MSc
Morton’s neuroma is a fairly common cause of foot pain that is reported far more frequently in females as compared to males (female to male ratio is 9:1). This high incidence is attributed mainly to the anatomy of female foot as well as lifestyle choices such as prolong use of narrow toe-box shoes or long hours of standing etc. Unfortunately, poorly managed foot pain can also aggravate the risk of developing other disorders such as bursitis.
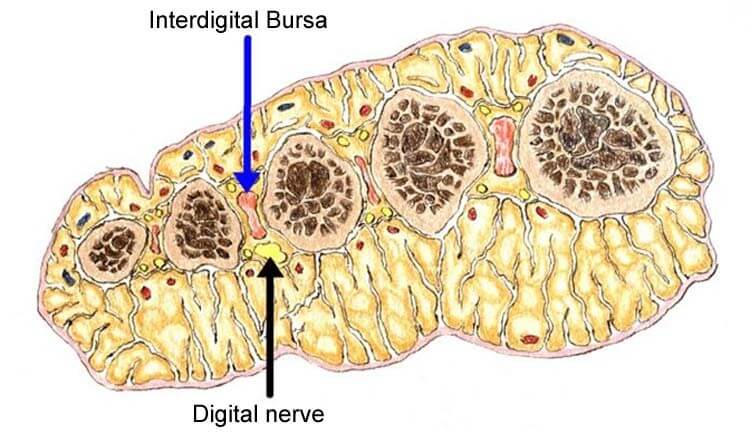
However, in some cases the two conditions may coexist asymptomatically i.e. without any pain or noticeable symptoms.
The diagnosis of Morton neuroma and bursitis is mostly clinical i.e. more than 85-90% cases can be identified on good history taking and clinical examination. For more complex or concealed cases, radiological tests like an ultrasound or magnetic resonance imaging (MRI) may be needed.
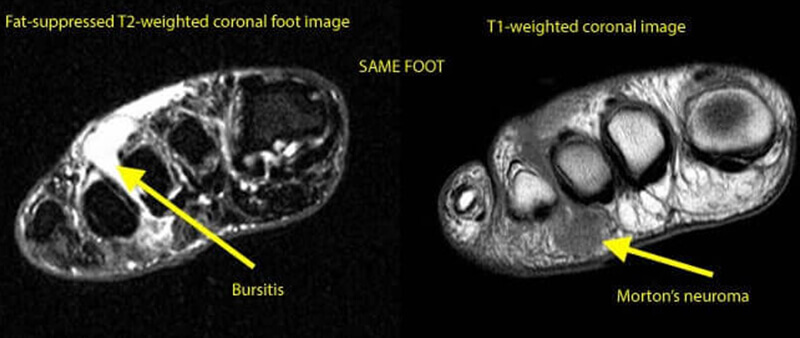
Bursitis can be differentiated from the Morton neuroma on scans via following features:
Generally no management or clinical workup is necessary if Morton neuroma is pain free and identified accidentally on physical examination. For painful or disturbing neuromas, the choice of therapy depends on overall health and patient factors.
Most common management tools to control the symptoms of these two conditions primarily revolves around:
In chronic cases:
References:
By providing us with your information you are consenting to the collection and use of your information in accordance with our Terms of Service and Privacy Policy.