Pain after Morton’s neuroma surgery is common and can be difficult to treat.

Some studies have shown that up to 35% of patients who have had Morton’s neuroma surgery end up with unacceptable levels of post surgical pain, also known as “post neurectomy pain”.
The exact cause of pain after Morton’s neuroma surgery can often be difficult to determine. It can even be difficult to localize the exact location of the pain after surgery. The pain can be the result of an incorrect initial diagnosis, inadequate surgical resection, or the occurrence of a stump neuroma.
Post Morton’s neuroma surgery (or post inter-metatarsal neuroma surgery) pain is usually due to a stump neuroma combined with nerve entrapment within the scar tissue that develops during postoperative healing. Post-surgical pain can also be due to nerve degradation or just plain scar tissue formation or rarely, another post surgical complication. Some authors speculate that disruption of the plantar fat pad during surgery may contribute to post Morton’s neuroma surgery pain.
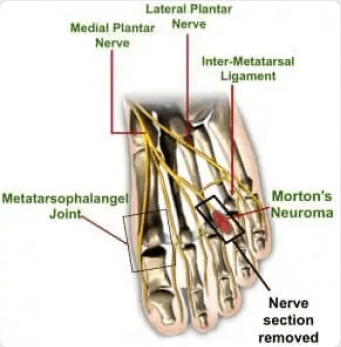
A stump neuroma is a traumatic, or amputation stump neuroma affecting the common digital nerve and is usually located just near (proximal) to the metatarsophalangeal joint. The stump, or traumatic neuroma develops as the budding nerve cells in the near section of the cut nerve trunk multiply and attempt to bridge the gap and grow towards the nerve trunk of the far segment of the cut nerve. The newly budding nerve cells become entrapped in scar tissue and may stick to neighboring structures, such as the metatarsophalangeal joint capsule, the bone surface (the periosteum of the metatarsal shaft), and nearby tendons, ligaments, and muscle. One of the most common causes of post Morton’s neuroma pain is the adhesion of the stump neuroma to one of the metatarsal heads.
Post surgical pain usually becomes apparent between three and eight weeks postoperatively, or it may develop after months, or even years of a seemingly successful surgical intervention. In general, if there is no improvement by three or four months after surgery there is probably little chance of further improvement.
It has been speculated that surgical technique during the initial Morton’s neuroma surgery causes most post Morton’s neuroma surgery pain.
During the initial Morton’s neuroma surgery (“neurectomy”), the nerve should be removed from about 3 cm below (“proximal to”) the inter-metatarsal ligament to a point about 1 cm down from (“distal to”) the bifurcation of the common digital nerve. The remaining nearby nerve ending (the proximal nerve stump) should be moved and buried into surrounding muscle tissue (i.e. into the adductor hallucis brevis) to prevent a stump neuroma forming.
In cases of Morton’s decompression surgery, the inter-metatarsal ligament is cut and the Morton’s neuroma is not removed but depending on the surgeon, the nerve may also be cut and buried.
Many surgeons use steroid, alcohol or dilute phenol infiltration into the proximal nerve stump to attempt to decrease the chance of a post surgical stump neuroma forming but these have not been proven to help. Some surgeons cap the proximal nerve stump with silicone during the operation but this has also yielded inconsistent results and very often requires reoperation to remove the silicone capping and revise the surgery.
Inadequate nerve trunk removal and inadequate nerve placement into the surrounding muscle is thought to be the most likely cause of Morton’s neuroma recurrence or stump neuroma. Unfortunately, there is no way to accurately measure the adequacy of the nerve trunk resection at the time of surgery, and the surgeon can only hope for a clean, sharp cut, with accurate anatomic dissection, correct nerve placement, absolute hemostasis, and the avoidance of any wound complications. The likelihood of the recurrence increases if the patient develops a postoperative infection or bruising.
The most common sign associated with recurrent Morton’s neuroma (also known as Morton’s metatarsalgia) is exquisite local tenderness at the level of the stump neuroma. The pain is usually nerve pain like (“neuritic”) in nature, with the patient complaining of sharp, burning, or electrical type pain. This is usually located about 1 to 1½ centimeters proximal to the metatarsophalangeal joint. Occasionally, patients will complain of a nodule or “lump” in the previously operated web space associated with scar tissue or bursitis.
Symptoms are typically aggravated by weight bearing, walking, and wearing certain shoes (usually shoes with high heels, narrow toe box, and thin soles.)
Tinel’s sign may be elicited upon direct dorsal (top of foot) or more commonly plantar (bottom of foot) palpation of the recurrent lesion. This finding, however, need not be present in all cases. Similarly, the web space may be numb or dull to touch.
The key finding is the reproduction of symptoms upon direct, deep palpation of the stump neuroma. The pain can be very debilitating and, at the least, often makes the patient alter his/her shoe gear if not lifestyle.
The diagnosis for post Morton’s neuroma surgery pain or for a recurrent neuroma can be difficult and care should be taken to rule out other causes of metatarsalgia, especially if the pain is dull in nature. The diagnosis should be made by a practitioner well experienced in assessing and treating Morton’s neuroma patients.
Special emphasis should be directed toward ruling out specific biomechanical problems of the forefoot that may or may not be directly related to the neuroma recurrence.
Arthritis affecting the metatarsophalangeal joints is frequently associated with painful articular subluxation, as well as synovitis of tendon sheaths, which could be mistaken for focal Morton’s neuroma pain. Careful palpation should be performed in an attempt to rule out the presence of a symptomatic intermetatarsal bursitis, plantar synovial cyst originating from the adjacent joint, or proliferation of synovium. Most of these inflammatory conditions will respond favorably to the use of non-steroidal anti-inflammatory drugs (NSAID’s) and/or glucocorticosteroids, whereas stump neuromas associated with deep, diffuse scarring usually do not.
The possibility of new neuroma formation in an adjacent webspace, or of an accessory nerve in the same interspace, should be considered.
Post surgical nerve entrapment of dorsal cutaneous nerves may also develop after surgery if a dorsal (top of foot) approach was used.
One should also carefully consider the possibility of a painful plantar scar as a cause of the patient’s symptoms, if a plantar approach was used. These usually presents as slightly hypertrophic, hyperkeratotic lesions, with palpably indurated subcutaneous tissues. The patient will often relate a history of immediate postoperative weight bearing following the first surgery.
Thinning of the plantar metatarsal fat pad with loss of shock absorbing capacity is a frequent complication of poor webspace surgical technique.
A failed first surgery will probably not respond to conservative treatment. Non-steroidal anti-inflammatory drugs are almost universally ineffective in alleviating post surgical pain or the pain of recurrent intermetatarsal neuroma. Modifications of shoes to include a low heel, wide toe box, and orthotics may give some temporary relief.
Local steroid or anesthetic ointments may be used for post-surgical nerve entrapment affecting the intermediate dorsal cutaneous and sural nerves. Painful scars often respond well to local anesthetic or steroid creams. Any use of local anesthetic or steroid creams should be supervised by a physician experienced in the use of these creams to avoid any harmful complications.
Similarly a steroid injection may be temporarily helpful, primarily due to its late stage fibrolytic effects. If you pursue this course of treatment, we suggest two or three local steroid injections, under ultrasound guidance, over a three to six month period as long as reasonable improvement is made following each injection. These should be combined with physical therapy with or without joint manipulation depending upon the individual patient’s degree of sensitivity. These measures may provide some temporary relief.
Usually patients who have post Morton’s neuroma surgical pain have had to modify their walk (or “gait”) to accommodate the pain. This frequently causes other problems such as back pain and joint pain. We recommend that all patients after receiving treatment for their post surgical pain receive orthotic insoles, either good off the shelf orthotics or even better custom orthotics to compensate for the gait issues and problems that have arisen from their coping with post surgical Morton’s neuroma pain. For more information on orthotics, click here.
Ablation procedures done under ultrasound can be very effective in alleviating post Morton’s neuroma surgical pain, assuming that one can accurately localize the source of the pain.
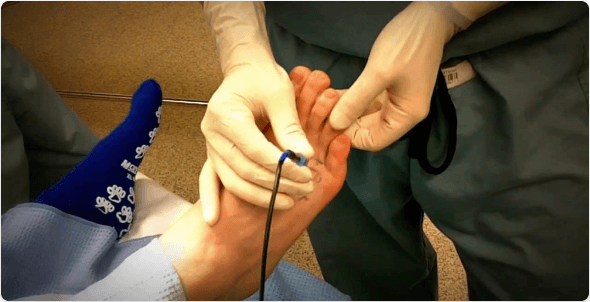
This usually requires a diagnostic local anesthetic injection done under ultrasound and preferably with nerve stimulator guidance beforehand, to ensure that the source of the pain can be accurately localized. This diagnostic injection also tests that the pain is responsive to local anesthetic which is an indication that the pain will respond well to an ablation procedure.
Once the source of the post surgical pain has been accurately localized and shown to respond to local anesthetic, then an ablation procedure can be performed. The ablation procedures that are available include radiofrequency ablation (“RF ablation”) under ultrasound guidance, cryoablation under ultrasound guidance and neurolytic injection under ultrasound guidance. You should discuss which procedure is most suitable for you with your practitioner. Given the complexity of post surgical Morton’s neuroma pain, these procedures should be performed by practitioners who are well versed and well experienced in these and they will probably need to be repeated as long as significant improvement is made following each procedure. For more information on ablation procedures see here.
Even when an ablation procedure is done after a positive diagnostic local anesthetic injection an accurate prediction of the outcome is difficult to make given the individual variability of exact cause of the pain.
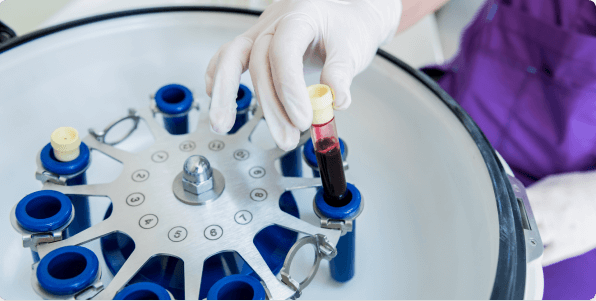
are very helpful for their effect on local inflammation which is frequently present in painful stump neuromas. Careful attention should be given to identify bursitis or synovitis both of which respond well to Platelet rich plasma injections. We routinely perform Platelet Rich Plasma Injections for all of our post Morton’s neuroma surgery patients who come with post surgery pain. We combine this with an ultrasound guided ablation procedure for best rests.

Approximately 15% of previously operated patients will elect to undergo another surgical intervention in an effort to alleviate recurrent pain, however some research papers have reported that 80% of these Morton’s neuroma surgery redos are unsuccessful.
The overall goals of re-operation are identification of the neuroma and any other pathologic structures, and clean sharp removal of the closer (“proximal”) nerve stump as far proximal as possible. Careful inspection must be made for any abnormal accessory nerves, bursae (especially in the second and third interspaces), synovial cysts, or localized scar in the interspace. Should there be any indication of the far (“distal”) nerve stump being entrapped then a sharp, clean distal removal of the that stump should also be done and the remaining stump should be moved to a well vascularized and well protected soft tissue bed.
The choice of surgical approach is a crucial preoperative consideration and should be carefully made by a surgeon well experienced in these procedures. A top of the foot approach is typically used for the first operation, resulting in some local scar tissue so a bottom of the foot (“plantar”) approach is most commonly used in revision surgeries. Caution should be practiced to avoid overly aggressive disruption of the shock absorbing plantar fat pad. However, any plantar approach will damage part of the plantar fat pad and result in some amount of scar tissue. For this reason, three weeks of non-weight bearing must be maintained after surgery. It usually takes 4-6 months post revision surgery to become fully mobile.
We recommend orthotic insoles for all patients post Morton’s neuroma revision surgery, either good off the shelf orthotics or even better custom orthotics to compensate for the gait issues and other problems that have arisen from their coping with their Morton’s neuroma pain and surgery. For more information on custom orthotics CLICK HERE.
Due to the variability of post Morton’s neuroma surgical pain, an accurate prediction of revision surgery outcome is difficult to make. Should your Morton’s neuroma not respond to our ablation procedures, Dr. Pearl will confer with you and surgical colleagues here in the Boston area hospitals for a possible surgical option and we will co-ordinate your care to try to ensure that you receive the best possible treatment.
By providing us with your information you are consenting to the collection and use of your information in accordance with our Terms of Service and Privacy Policy.