Did you know that females are 8-10 times more likely to develop Morton’s Neuroma as compared to males(1)? Some research articles claim Morton’s neuroma has an 18 to 1 female to male ratio(2)!!
It is true that more females develop Morton’s neuroma each year when compared to males due to anatomical, physiological or lifestyle choices.
Morton’s neuroma is often described as a chronic painful neuralgia (nerve pain) that involves the fore-foot. Contrary to the common belief, Morton’s neuroma is not a typical nerve tumor, in fact it is caused by nerve degeneration and thickening of plantar digital nerve due to entrapment or exposure to chronic pressure. In poorly managed situations, the nerve undergoes fibrotic changes. Patients present with:
Needless to say that Morton’s Neuroma can alter the overall quality of life by interfering with personal, professional and social aspects of your life.

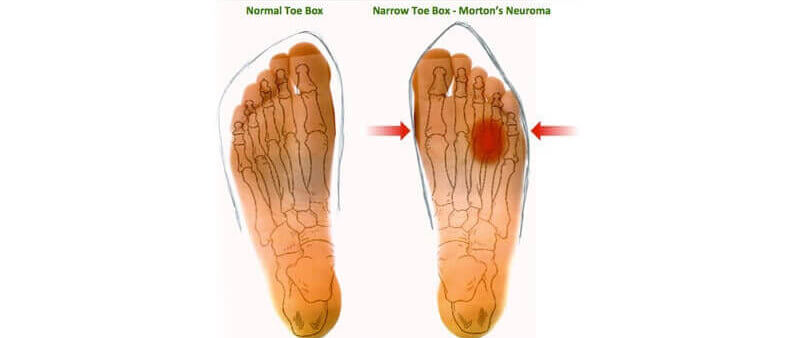

According to a new study reported in the peer reviewed journal Clinical Drug Investigation (1), Morton’s Neuroma is strongly associated with ‘overload mechanism’ in the forefoot. For example, overcrowding of metatarsal bones due to anatomical variations (such as congenital or acquired bone deformities) or poor choice of footwear can lead to irritation of delicate nerves that are responsible for pedal sensations. Females are at much higher risk because the anatomical construction of a female foot is different from a male foot. For example, experimental study reported in the Journal of the American Podiatric Medical Association (3) suggested that feet in males are inherently much stronger and longer than an average female (with similar demographic profile). Additionally as compared to males, female feet are inherently higher and narrower that poses metatarsals to pressure and strain (thus explaining why females develop this condition more frequently). Some key differences between male and female foot are:
Additionally more women are likely to wear high-heels or pointed shoes as compared to males. For a details description of the science behind Morton’s neuroma, click here.
Morton’s neuroma is responsible for 7.8% of all the podiatric surgeries performed in clinical practice each year(4); however, early management can significantly reduce the risk of surgical intervention by 80%(5). Experts also suggest that dynamic (or physically active) females should specifically consider sports gear and covered shoes that are designed for females (instead of using uni-gender shoes or footwear).
These days there are many procedures that can be performed to cure Morton’s neuroma without the need for surgery such as ultrasound guided radio frequency ablation(6), ultrasound guided cryo-ablation(7), and ultrasound guided neurolytic injections(8),(9).
If you have Morton’s neuroma, you should see a physician experienced in the treatment of Morton’s neuroma and experienced with these procedures. For More information on these procedures, click here.
References:
Climent, J. M., Mondéjar-Gómez, F., Rodríguez-Ruiz, C., Díaz-Llopis, I., Gómez-Gallego, D., & Martín-Medina, P. (2013). Treatment of Morton Neuroma with Botulinum Toxin A: A Pilot Study. Clinical drug investigation, 33(7), 497-503.
Goud, A., Khurana, B., Chiodo, C., & Weissman, B. N. (2011). Women’s musculoskeletal foot conditions exacerbated by shoe wear: an imaging perspective. Am J Orthop, 40(4), 183-191.
Luo, G., Houston, V. L., Mussman, M., Garbarini, M., Beattie, A. C., & Thongpop, C. (2009). Comparison of male and female foot shape. Journal of the American Podiatric Medical Association, 99(5), 383-390.
Bennett, P. J. (2007). Prevalence and type of foot surgery performed in Australia: A clinical review. The Foot, 17(4), 197-204. http://www.sciencedirect.com/science/article/pii/S0958259207000478
https://www.podiatry.com/etalk/Mortons-Neuroma-Four-out-t6915.html#-1
Chuter GS1, Chua YP, Connell DA, Blackney MC. (January 2013). “Ultrasound guided radiofrequency ablation in the management of interdigital (Morton’s) neuroma”. Skeletal Radiol. 2013 Jan;42(1):107-11. doi: 10.1007/s00256-012-1527-x. Epub 2012 Oct 17. 42 (1): 107–11.
Talia Friedman, MD, Daniel Richman, MD and Ronald Adler, MD, PhD. “Sonographically Guided Cryoneurolysis Preliminary Experience and Clinical Outcomes”. J Ultrasound Med 2012; 31:2025–2034.
Hughes RJ, Ali K, Jones H, Kendall S, Connell DA. (June 2007). “Treatment of Morton’s neuroma with alcohol injection under sonographic guidance: follow-up of 101 cases”. Acta Orthop Belg. 2007 Apr;73(2):224-9 188 (6): 1535–9.
Musson RE1, Sawhney JS, Lamb L, Wilkinson A, Obaid H. (March 2012). “Ultrasound guided alcohol ablation of Morton’s neuroma”. Foot Ankle Int. 2012 Mar;33(3):196-201.
By providing us with your information you are consenting to the collection and use of your information in accordance with our Terms of Service and Privacy Policy.