(Etiology, Pathogenesis, Location, Disease Progression and Histology)
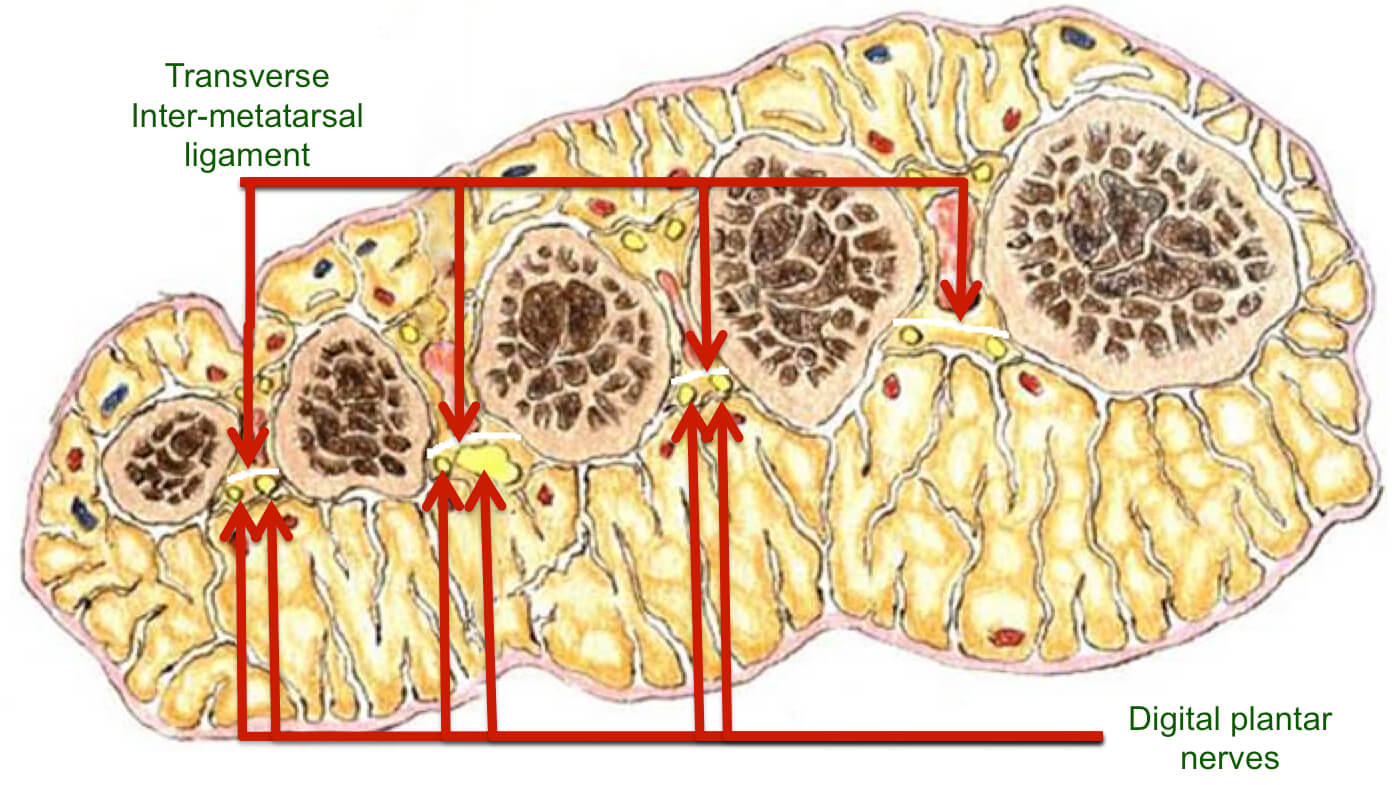
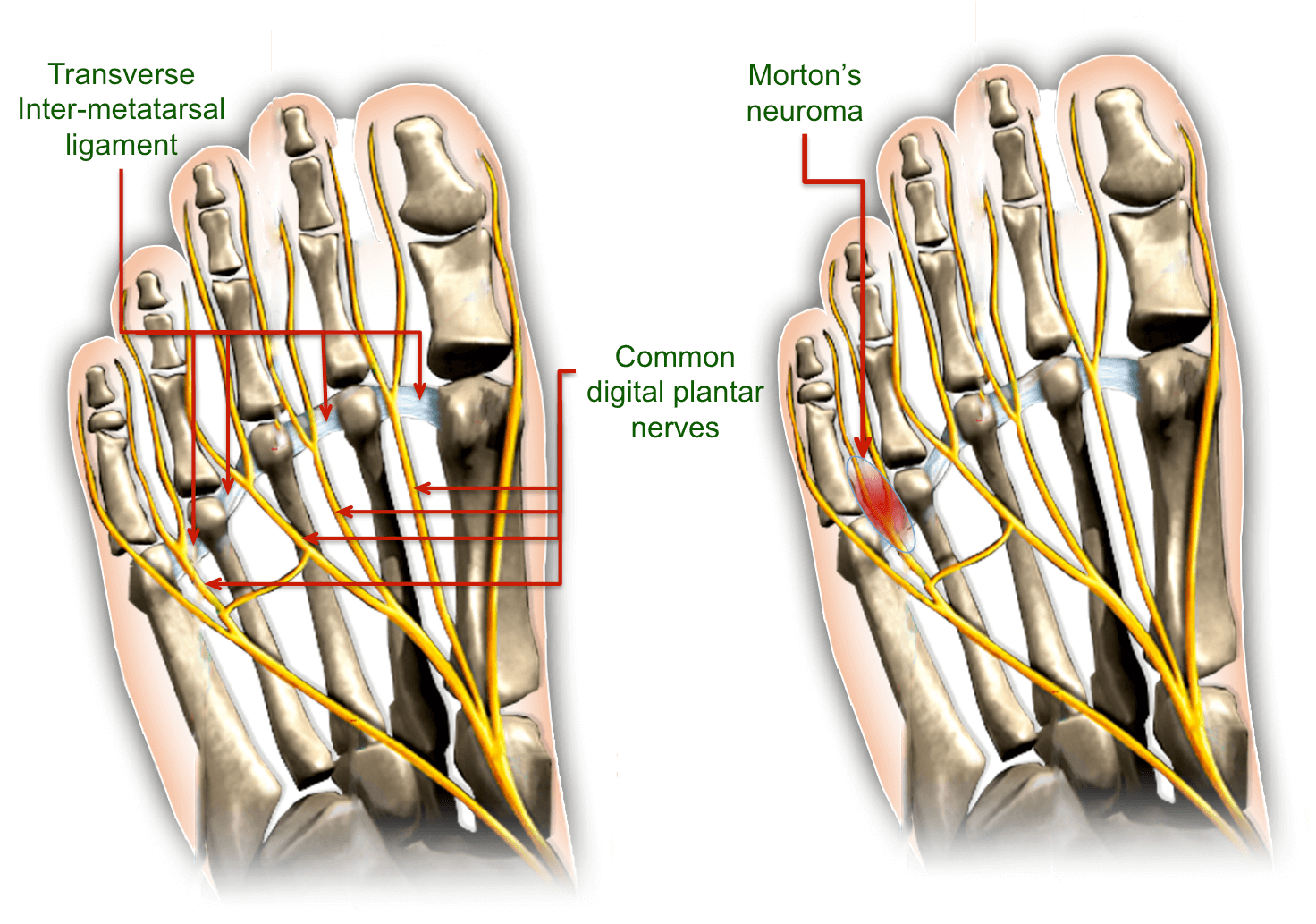
The exact cause of Morton’s Neuroma (also known as Morton’s metatarsalgia, Morton’s neuralgia, plantar neuroma and intermetatarsal neuroma) is unclear. We believe that Morton’s neuroma is the result of a combination of a chronic low-grade compression trauma and a classic ischemic entrapment neuropathy of the common digital plantar nerve at its bifurcation point. Due to factors relating to gait and tight shoes, the common plantar digital nerve is repeatedly squeezed between the plantar aspect (the bottom) of the foot and the anterior distal edge of the transverse inter-metatarsal ligament.[i] The result is a chronic irritation of the nerve and the subsequent development of a benign fibrotic neuroma within the nerve.
An element of inflammation in the adjacent bursitis is frequently present and may contribute to symptoms as well.
The exact pathogenesis of how an entrapped digital plantar nerve results in Morton’s neuroma pain is not known and is the subject of much debate. Most investigators consider it to be an entrapment neuropathy,[ii] specifically direct pressure on the nerve leading to a chronic fibrotic reaction.[iii]
However, some studies show that chronic repetitive low-grade trauma is also present and conclude that Morton’s neuroma is due to a chronic mechanical overload of the entire webspace.[iv] The position of the neuroma, relative to the transverse intermetatarsal ligament suggests repetitive compression and/or friction against the anterior margin of the ligament during the push-off phase of walking[v]. Relief is often obtained by taking off the shoe and manipulating the forefoot.
These two are not mutually exclusive and we believe that Morton’s neuroma is due to a combination of chronic mechanical trauma of the webspace and an entrapment neuropathy of the nerve. Histological findings show evidence of both etiologies. See Histology below.
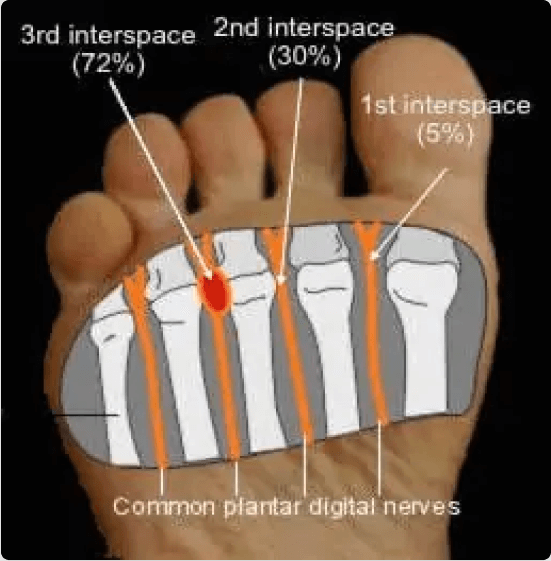
Morton’s neuroma occurs most commonly in the third interspace (72% of cases) followed by the second (30% of cases) and the fourth (5% of cases). Please note that these numbers add up to more than 100% due to multiple neuromas. The cause of the increased incidence in the third intermetatarsal space is unknown but it is thought that the following factors may be contributing:
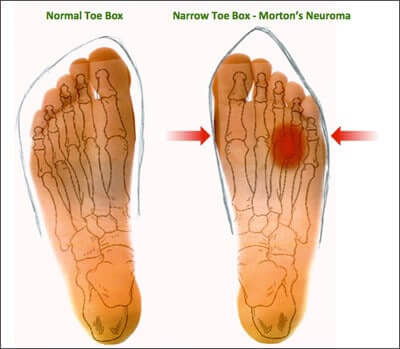
Morton’s neuroma occurs more frequently in women (78% of cases) and in athletes. Shoes with narrow toe boxes cause increased pressure by compression of the forefoot, especially when combined with gait abnormalities. It is speculated that women wearing high-heeled shoes increase the likelihood of Morton’s neuroma by:
The entrapment injury may also be affected by other factors. In up to 80% of patients, intermetatarsal neuroma may be associated with some other pathological findings of the forefoot such as hallux valgus (bunion), hammer-toe, or pes transversus (splay foot) where the transverse arch of the foot is lowered so that the heads of the metatarsal bones II – IV stand lower.
The webspace is fairly small and tight. Due to the mechanical forces mentioned above, the common digital nerve is trapped and squeezed between the intermetatarsal ligament and the dorsum of the foot. This chronic mechanical overload causes a mucoid degeneration of the intermetatarsal space frequently extending into the bursa. The increased tissue volume caused by accumulated mucoid ground substance within the confined intermetatarsal web space results in increased pressure and increased mechanical forces.
Furthermore, the compressed nerve causes reduced blood flow in the vessels supplying the nerve with blood (the vasa nervorum). This causes local ischaemia, which decreases the ability of the nerve axons to transmit. As the compression becomes more severe over time, focal demyelination occurs, followed by axonal damage and finally, fibrotic scarring within the nerve.
As the fibrosis continues, the fibrotic mass within the nerve progressively enlarges leading to greater entrapment and increased frictional forces.
Morton’s neuroma is a fusiform enlargement of the plantar digital nerve at its bifurcation point with a thickening of the adjacent tendosynovial tissues.
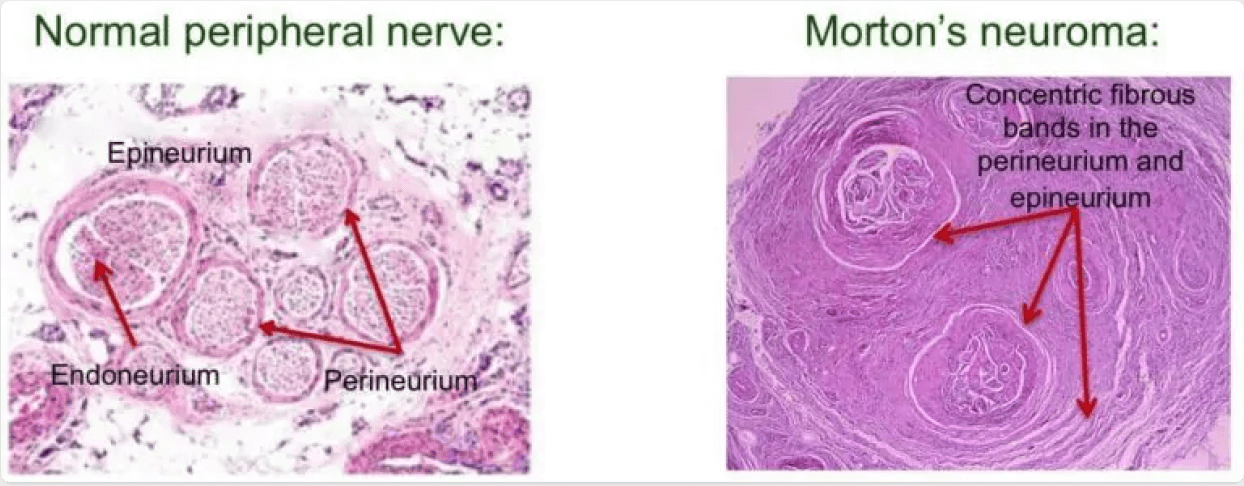
Microscopically, degenerative changes are the hallmark of Morton’s neuroma. Initially, the nerve shows fusiform swelling caused by the deposition of amorphous eosinophilic material. Edema and fibrosis occurs within the nerve, specifically within the epineurium and perineurium. As the lesion progresses, epineural and perineural fibrosis becomes increasingly prominent and envelops the epineurium and perineurium of the nerve in a concentric fashion. This dense fibrosis occasionally invades the endoneural space and is combined with a loss of myelinated nerve fibers.
Small vessels changes also occur. Fibrosis, thickening and hyalinization of the walls of endoneurial vessels are frequently present and there may be fibrointimal thickening with occlusion of small blood vessels. These enarteritis changes are characteristic of an ischemic entrapment neuropathy.
Mucoid degeneration (which histologically stains with alcian blue) is frequently seen in the fibroadipose tissue adjacent to the Morton’s neuroma often extending into the synovial lining of the intermetatarsal bursa. Frequently, the bursa also shows fibrinoid degeneration. In some cases bursitis may also be present. The mucoid degeneration in the intermetatarsal space is indicative of a connective tissue response to chronic repetitive low-grade trauma such as the trauma that would result from a mechanical overload in the webspace due to a nerve entrapment.
Identical fibrotic changes are observed in asymptomatic Morton’s neuroma[vi] (confirmed in cadaveric studies.) However, there is a greater degree of demyelination in patients with symptomatic Morton’s neuroma versus those with asymptomatic Morton’s neuroma suggesting that the demyelination is related to the pain. Surprisingly, it is not uncommon for the histopathology to be interpreted as relatively normal, even when a Morton’s neuroma was surgically excised and resulted in a dramatic reduction of pain.
We don’t know what causes the pain of Morton’s neuroma. It is not known whether the pain experienced by Morton’s neuroma is due to the increased intermetatarsal webspace pressure, the mechanical irritation from the chronic webspace overload or the demyelination of the common plantar digital nerve.
Identical histomorphological and fibrotic changes are observed in both symptomatic and asymptomatic Morton’s neuroma patients[vi]. This confirms that these changes are not the cause of pain. In other words, the pain that is typical of Morton’s neuroma cannot be explained by the size of the Morton’s neuroma nor by the degree of the histological findings. A large Morton’s neuroma with significant histological changes may be asymptomatic while a small Morton’s neuroma with minor or no histological changes may be extremely painful.
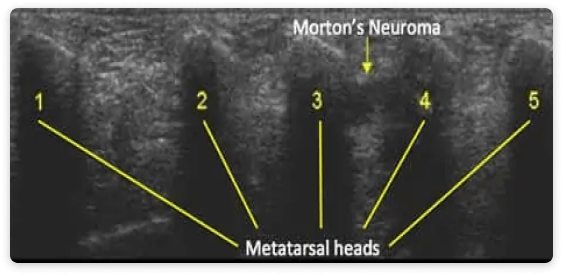
MRI or ultrasonography should only be used for diagnostic purposes, and even then they should be used in conjunction with a thorough history, physical examination and possibly diagnostic tests under local anesthesia. MRI or ultrasonography are not a reliable indicator of conservative versus operative treatment.[vii],[viii]
Due to the fact that the size of the Morton’s neuroma is not correlated to the symptoms, neurolysis (the killing of the nerve) is effective and recommended as the preferred treatment rather than neurectomy (the removal of the nerve,) especially since neurolysis preserves the integrity of the transverse intermetatarsal ligament, which is important for foot stability.
The correct treatment plan for each patient should always be formulated by a physician experienced in Morton’s neuroma and based on a thorough evaluation of the patient, taking into account the patient’s past history, past treatments and careful clinical evaluation.
We offer a number of procedures to treat Morton’s neuroma without surgery. To see the treatments we offer for Morton’s neuroma click here.

By providing us with your information you are consenting to the collection and use of your information in accordance with our Terms of Service and Privacy Policy.